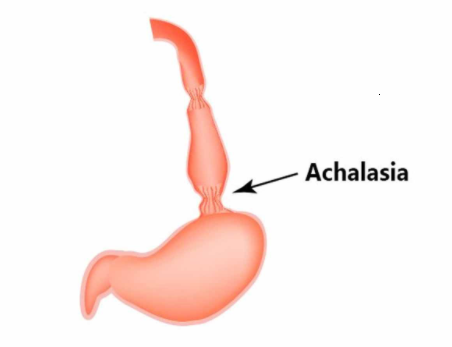
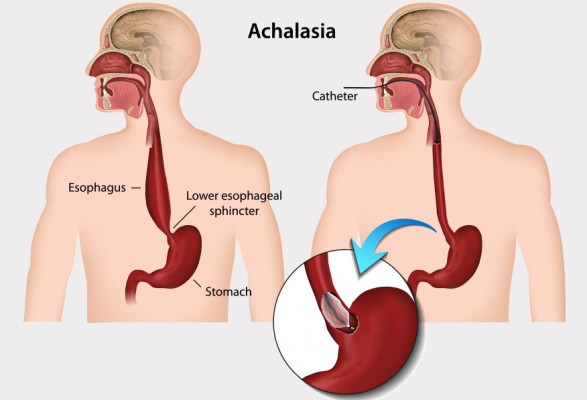
Internal achalasia is rare due to which the esophagus is unable to transfer food and fluids to your stomach. The esophagus is a muscular tube that carries food from the mouth to the stomach. Where your esophagus meets your stomach is a ring of muscle called the lower esophageal sphincter (LES). This muscle relaxes and allows food to enter the stomach and then contract. It prevents the stomach from contracting in the esophagus. In a patient with achalasia, the sphincter does not relax, preventing it from moving inside your stomach.
What causes achalasia?
It is not clear why human esophageal muscles do not contract and relax naturally. According to one theory, achalasia is an autoimmune disease caused by a virus. The immune system attacks the nerve cells in the muscular layers of the esophageal wall and the sphincter muscle. The nerve cells that control muscle function are slowly degenerating. The cause of this problem is not known, but it can lead to excessive contraction of the sphincter muscle. So if you have achalasia, food and fluids cannot pass through your esophagus into your stomach. According to another theory, the cause of achalasia can be hereditary. But more research is needed.
Symptoms of achalasia
Difficulty swallowing (most common early sign)
Return undigested food
- Chest pain
- Heartburn
- Weight Loss
- Malnutrition
- Hiccups and sore throat
Standard treatments
There are several treatments for achalasia, including non-surgical options (balloon dilation, medications, and botulinum toxin injections) and surgical options. The goal of treatment is to relieve your symptoms by relaxing the lower esophageal sphincter (LES).
Minimally invasive surgery
The surgery used to treat achalasia is called laparoscopic esophagomyotomy or Heller’s laparoscopic myotomy. In this minimally invasive surgery, a thin, telescopic instrument called an endoscope is inserted through a small incision. The endoscope is attached to a small video camera – smaller than a coin – that displays the view of the operating site on video monitors in the operating room. In this operation, the LES muscle fibers are cut. Adding another method called partial fundoplication helps prevent gastric reflux into the esophagus, a side effect of Heller’s myotomy.
Balloon dilation
In this non-surgical procedure, you undergo light relaxation while a specially designed balloon is inserted through the LES and then inflated. This method relaxes the muscular sphincter, which allows food to enter your stomach. Balloon dilatation is usually the first treatment option in people who fail surgery.
You may need to do several dilation treatments to relieve your symptoms and every few years to maintain relief.
medicine
If you are not a candidate for balloon dilation or surgery or do not decide to have these procedures, you may benefit from Botox injections (botulinum toxin). Botox is a protein made by bacteria that cause botulism. When Botox is injected into the muscles in very small amounts, it can relax the spastic muscles. It works by blocking the signal from the nerves to the sphincter muscles, which tells them to contract. The injection should be repeated to maintain control of symptoms.
Other medications include nifedipine (Procardia XL®, Adalat CC®) or isosorbide (Imdur®, Monoket®). These drugs relax the esophageal spastic muscles by lowering the LES pressure. These treatments are less effective than balloon surgery or dilation and only relieve your symptoms in the short term.
Esophagectomy
An esophageal resection is the last resort.